
Kristian Thorborg on Prevention of Groin Injuries in Sport
- Jo Clubb

- Oct 21, 2015
- 5 min read
Updated: Oct 4, 2024
This article is the forth and final in a series of posts summarising Performance and Injury lectures from leading Sports Scientists.
Dr Kristian Thorborg is an Associate Professor and Physiotherapist based at the Sports Orthopaedic Research Centre. He has special interests in knee, hip and groin injuries and presented on ‘The Prevention of Groin Injuries in Sport’.

Understanding the Clinical Entity
Groin pain presents itself in a number of different clinical entities and so four main categories have been proposed with their prevalence given in brackets:
Adductor related groin pain (50-70%)
Abdominal related groin pain (5-20%)
Psoas related groin pain (10-20%)
Hip related groin pain (5-10%)
Pain can be caused by more than a single clinical entity and sometimes the prevalence of more than one, such as abdominal injury as well as adductor related groin pain, can add to the injury time. Due to the complex adductor abdominal synergi, in which different structures share the same insertion, this has implications for assessment via palpation and emphasises the need for careful assessment in the High Performance environment.
Sport Specific Injury Aetiology
Ice Hockey
Chang et al (2009) used EMG to assess muscle activity during different skating velocities and found with increasing speed there was an increase in stride rate, stride length, angular velocity and muscle activity. The adductor magnus peaked in activity during the transition phase from hip abduction to adduction during the stride.
This research helps to demonstrate the function and stress on the adductor muscle group during skating, particularly with a view to increased skating speed. Therefore attempting to monitor skating speeds and workload above certain speed thresholds in ice hockey may be an important process in trying to prevent groin pain and injury in this sport.
Due to the prevalence within the sport, researchers have looked into hip strength and asymmetries in relation to injury prediction as far back as 1973! For instance:
Hip strength asymmetries of more than 25% related to adductor strain on the weaker side (Merrified and Cowan, 1973)
Eccentric hip muscle strength as a ratio less than 0.8 was a predictor of hip adductor injury with as much as a 17 fold greater injury risk (Tyler et al, 2001)
However, isometric hip muscle strength was not a predictor (Emery et al, 2001)

Soccer
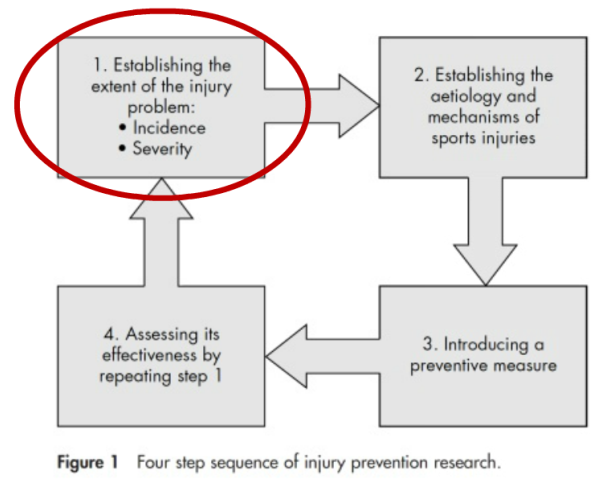
As another sport that suffers from a high prevalence of groin pain, research has also looked into the mechanisms and risk factors within soccer and Dr Thorborg presented a number of findings. If we consider the second step of injury prevention, establishing the aetiology and mechanism, Charnock and colleagues (2009) showed high muscle activation and high rate of stretch both occur at about 40-50% of the swing phase of a football kick. Both of these mechanisms are necessary for a muscle injury and may help to explain the high risk associated with soccer.
Obviously avoiding this kicking mechanism in soccer is not possible! So how can we measure and monitor the risk factors? It seems weakness is a risk factor for groin pain in soccer as a fourfold higher risk was shown to be associated with weakness (Engebretsen et al, 2010).
However, ‘weakness’ is a complex construct and I think we need to consider what weakness in our own athletes actually means. Dr Thorborg presented contradictory findings in the literature that isometric testing is (Nevin and Delahunt, 2013) and is not (Thorborg et al, 2014) associated with groin pain. Once again, we may apply these tests within the High Performance environment and assess their association with groin pain and injury with our specific application but it is important to conduct a mini audit of our own tests and strategies to review which are making a difference to the programme.
Rugby
A common theme of Dr Thorborg’s discussion was to always frame the thoughts and findings within the injury prevention model for the specific sport. Moving onto rugby, whilst hip adduction and abduction strength and moments are not directly associated with side cutting performance, their primary function is to stabilise the hip during such movements (Marshall et al, 2014). Furthermore due to the complex synergi there are implications of pelvic tilt and rotational movements around the hip on these structures. A prediction model of 8 risk factors of groin injury and rugby did include hip adductor and abductor peak torques (O’Connor, 2014). So it does seem the groin structures can be vulnerable during the demands of rugby and therefore prevention strategies should be considered for this sport.
Groin Injury Risk Factors
As discussed across these sports the risk factors for groin pain include weak adductors, a reduced eccentric hip adduction:abduction strength ratio and previous injury. A key point in this discussion was the complexity of groin pain due to the structure of the anatomy in this area, across the anterior, posterior, and medial-lateral muscle synergis. Forces from the femur during sport are distributed around this pelvic ring but is the athlete able to dissipate these forces around the pubic symphysis? So we need to reflect on how we can build athletes who can cope with this.
Hip and Groin Injury Prevention
Dr Thorborg put forward two key ideas to best protect the muscle-tendon-bone unit and try to prevent injury:
Careful monitoring of load
Preparing athletes for specific and repetitive load and overload
There is evidence to support plyometric training as a prevention strategy as it increases EMG preactivity prior to ground contact (Chimera et al, 2004). Dr Thorborg emphasised just how adaptable the neuromuscular system as this study design over required plyometric training twice a week for six weeks.
I think it is really important to consider the practicality of adding prevention programmes to the High Performance programme as time can be limited and weighing up the cost to benefit balance. However, in this case it seems a relatively small amount of time needs to be invested to see an improvement so may be worthwhile in sports with a high prevalence of groin pain.
One of the key messages of this discussion was how understudied the prevention of groin injury is. There has only been 1 randomised controlled trial where preventing groin injury was the primary target (Holmich et al, 2010). This study suggested a prevention programme decreased the probability of experiencing a groin injury, although the results were not statistically significant.
However, this research group has now reflected on this programme and considered if the exercises used previously were specific and/or intense enough, so research has now emerged studying the EMG activity of different exercises (Jensen et al, 2012; Serner et al, 2013; Brandt et al, 2013; Jensen et al, 2014).
Whilst surface EMG has its limitations especially with measuring the activity of the deep muscles, I think it is really interesting to see the objective classification of exercises and this of course has implications for exercise selection in prevention and rehabilitation in the High Performance environment.
Finally, Dr Thorborg emphasised that when it comes to groin injury incidence we are only seeing the tip of the iceberg as when we use time lost in injury surveillance studies we are not capturing all groin pain and injury. Especially if you consider the following:
50% of soccer players have hip and/or groin pain during the season
Of those, 30% have pain for more than six weeks
Plus 30% bring their pain into next season.
This research group have tried to think differently about groin pain and injuries by developing the HAGOS score (http://www.koos.nu/HAGOSenglish.pdf).
We can certainly conclude that groin pain and injury is a prevalent issue across a number of sports in which injury incidence is being underreported and injury prevention is understudied. This may put onus on practitioners in the High Performance environment to perhaps lead on some of this research as they can truly capture groin pain by having full time access to their athletes.



Comments